Autophagy, Fasting, and Human Health: What the Evidence Actually Shows
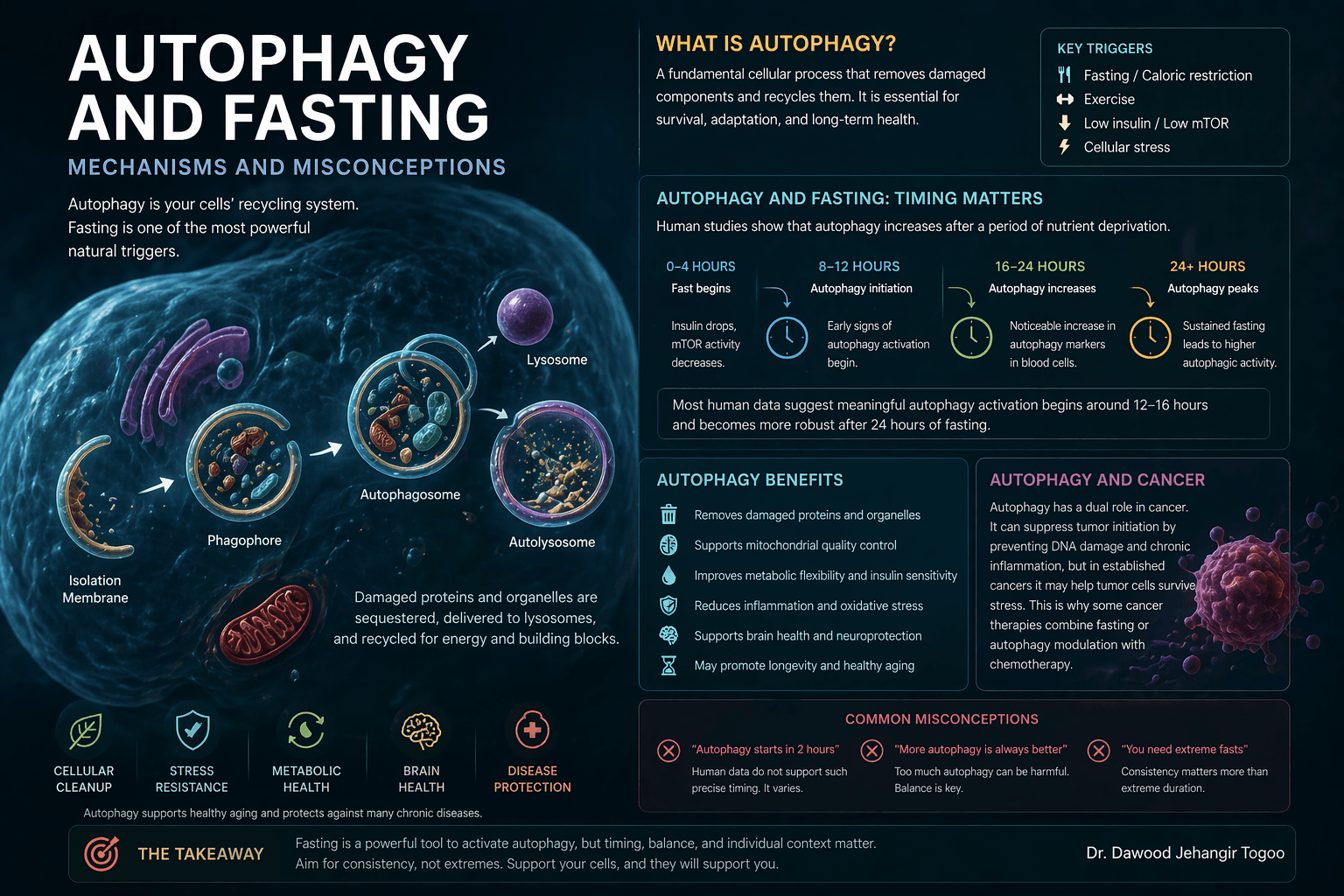
Autophagy is the cell’s internal recycling system. It helps break down damaged proteins, worn-out organelles, and other cellular material so that these components can be cleared or reused. In basic biology, this process is essential for cellular housekeeping, stress adaptation, and metabolic survival. That part is not controversial. What is controversial is how confidently people talk about fasting as a precise tool for turning autophagy on in humans.
The mechanistic logic is strong. When nutrient availability falls, insulin signaling declines, energy stress rises, AMPK activity increases, and mTOR activity falls. This combination creates a biochemical environment that favors autophagy. Much of that pathway is well established in experimental biology. The problem is not whether autophagy exists. The problem is that directly measuring meaningful, tissue-level autophagy in living humans is difficult. That is why many confident online statements about the exact timing of autophagy are stronger than the evidence allows.
What human studies actually show
Human evidence does exist, but it is still limited. One of the earlier important studies showed that fasting in human volunteers altered blood-cell biology in a way consistent with fasting-induced cellular stress responses, including reduced protein acetylation in white blood cells. That study supported the idea that fasting measurably changes pathways linked to autophagy in humans, but it did not establish a universal hour-by-hour autophagy timetable for the whole body.
More direct human data arrived in a 2025 pilot randomized trial of a fasting-mimicking diet in healthy adults. In that study, researchers measured autophagic flux in peripheral blood mononuclear cells and found significant between-group differences by the end of the intervention, alongside changes in fasting glucose, beta-hydroxybutyrate, and HOMA-IR. This is important because it goes beyond theory and actually measures a human autophagy-related endpoint. At the same time, it was a small pilot study, measured blood cells rather than all tissues, and does not justify sweeping claims that every person reaches maximal autophagy at the same fasting duration.
Another 2025 human study reported that intermittent time-restricted eating may increase physiological autophagic flux in peripheral blood. Taken together, the emerging human literature suggests that fasting can increase autophagy-related activity, but the best evidence so far is still blood-based, relatively early-stage, and not precise enough to define a single “correct” fasting window for all people.
So what fasting window is optimal for autophagy
This is where most internet advice becomes overstated. Based on current human data, there is no universally proven optimal fasting length for autophagy. The strongest statement we can make is that autophagy-related biology appears to become more likely as the fast deepens, particularly once insulin is low, glycogen availability is reduced, and ketones begin to rise. In practical terms, that means a longer fast is generally more biologically plausible for autophagy-related effects than a short overnight fast, but the human literature does not let us assign a single precise threshold such as 12 hours, 16 hours, or 24 hours for everyone.
If the goal is metabolic health, the evidence base is better for structured time-restricted eating than for chasing a supposed autophagy clock. A 2025 meta-analysis found that 16:8 time-restricted eating improved fasting glucose, fasting insulin, and HOMA-IR overall, though the effects varied and were more convincing in some subgroups and with longer study duration. In addition, early time-restricted feeding, where food intake is confined earlier in the day, improved insulin sensitivity and beta-cell responsiveness in men with prediabetes even without weight loss.
A reasonable evidence-based interpretation is this. For general metabolic benefit, eating within roughly a 6 to 10 hour daytime window may be useful for many people. For autophagy specifically, longer fasting exposures may produce stronger signals, but the human evidence is not yet good enough to define an exact optimum.
Autophagy and insulin
This is one of the clearest clinically relevant parts of the fasting literature. Fasting reduces insulin exposure, and lower insulin signaling is one of the major molecular conditions that favors autophagy. In parallel, fasting interventions often improve insulin sensitivity, especially in people with impaired metabolic health. The 2025 16:8 meta-analysis showed overall improvement in fasting glucose and fasting insulin, with a probable slight reduction in HOMA-IR as well.
The 2018 early time-restricted feeding trial is also important here because it suggests that some of the insulin-related benefits of fasting are not merely a side effect of losing weight. In that study, insulin sensitivity improved even without weight loss. That makes the physiology more interesting. Fasting may improve metabolic signaling not only by reducing calories, but also by altering timing, circadian alignment, and time spent in the postabsorptive state.
This matters because insulin and autophagy are closely linked. In broad terms, lower nutrient and insulin signaling removes one of the brakes on autophagy-related pathways. That does not mean more fasting is always better. It means that insulin biology is one of the clearest mechanistic bridges between fasting and autophagy.
Does autophagy fight cancer
It is scientifically reasonable to say that autophagy can help protect cells from accumulating damage, and in that sense it may contribute to tumor suppression in early disease biology. But it is equally important to say that once cancer is established, autophagy can sometimes help malignant cells survive nutrient stress, hypoxia, and treatment. In other words, autophagy can both suppress and support cancer depending on the stage and context.
That dual role is well recognized in the oncology literature. It is also the reason some cancer strategies aim to promote fasting-like stress in certain settings, while others aim to block autophagy in established tumors. The biology is not one-directional.
So the evidence-based position is this: fasting and autophagy are biologically interesting in cancer research, and they may influence treatment response in some contexts, but they should not be marketed as proven anti-cancer therapies for the general public. Human oncology data are still developing, and cancer patients should not undertake major fasting regimens without specialist guidance.
What people get wrong about autophagy
The first mistake is pretending that autophagy has a universal timetable in humans. It does not. The second is assuming that more autophagy is always better. Biology is about regulation, not extremes. The third is treating fasting as if it were a substitute for medical treatment, particularly in cancer. That is not supported by current evidence.
The more scientifically honest view is that fasting can move human physiology toward an autophagy-favoring state, especially as fasting duration increases and insulin falls. But the exact timing, magnitude, and organ-specific relevance remain incompletely defined in humans. What is clearer today is the metabolic side: fasting patterns, particularly time-restricted eating, can improve insulin-related outcomes in many studies.
The high-yield takeaway
Autophagy is real, important, and strongly linked to nutrient deprivation biology. In humans, fasting does appear to promote autophagy-related pathways, but direct evidence is still limited and does not support a single exact fasting duration for everyone. If your goal is better metabolic health, the strongest human evidence currently favors consistent time-restricted eating and improved insulin sensitivity. If your goal is maximal autophagy, the science is promising but not precise enough yet to justify rigid claims. And if the topic is cancer, autophagy should be treated as a complex biological process, not a miracle narrative.
References Espinoza SE, et al. Effect of fasting-mimicking diet on markers of autophagy and metabolic health in human subjects. 2025. Pietrocola F, et al. Metabolic effects of fasting on human and mouse blood in vivo. 2017. Bensalem J, et al. Intermittent time-restricted eating may increase autophagic flux in peripheral blood. 2025. Wong P, et al. Effect of 8-Hour Time-Restricted Eating (16:8 TRE) on Glucose Metabolism and Lipid Profile in Adults: A Systematic Review and Meta-Analysis. 2025. Sutton EF, et al. Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes. 2018. Wolska W, et al. The Role of Intermittent Fasting in the Activation of Autophagy and Its Implications in Cancer Treatment. 2025. Mohammed WH, et al. The dual role of autophagy in suppressing and promoting cancer. 2024. Hassan AMIA, et al. Blockage of Autophagy for Cancer Therapy. 2024.
Dr. Dawood Jehangir Togoo